Fixed drug reaction
| Fixed drug reaction | |
|---|---|
| Other names: Fixed drug eruption | |
.jpg.webp) | |
| Fixed drug reaction | |
| Specialty | Dermatology |
| Symptoms | One or several red/purple skin patches in same location every time a particular drug is taken,[1] typically on face, lips, groin[2] |
| Usual onset | Around 2 hours after taking drug,[1] can be 2 weeks[3] |
| Causes | Type IV hypersensitivity,[4] antibiotics, non-steroidal anti-inflammatory drugs[4] |
| Diagnostic method | History, visualisation, skin biopsy, oral challenge test, patch test[4] |
| Differential diagnosis | Insect bite reaction, bullous pemphigoid, erythema multiforme, Stevens-Johnson syndrome, herpes simplex, aphthous ulcer[4] |
| Treatment | Identify and stop causative drug, topical corticosteroid[4] |
| Frequency | Common, males=females, age 35-60 years[3] |
A fixed drug reaction is a rash that appears in the same fixed location every time a particular drug is taken.[1] It is typically a solitary well-defined, roundish red or purplish patch.[1][2] There may however be several which can be scattered or generalized, and there may be blisters, vesicles, erosions or ulcers.[3] It can be itchy and painful and often leaves a dark mark after healing.[4] Common sites include face, lips, groin, hands, feet, eyelids, anogenital areas, tongue and hard palate.[2][4]
It is a delayed type IV hypersensitivity, usually caused by antibiotics and non-steroidal anti-inflammatory drugs.[4] A typical time from taking the drug to noticing the rash is around 2 hours,[1] but can be 2 weeks.[3] Diagnosis is by history and visualisation of the rash.[3] It may require a skin biopsy, oral challenge test with a low dose of the suspected drug or a patch test.[4] The first epiode may be mistaken for an insect bite reaction or bullous pemphigoid.[4] Other differentials include erythema multiforme, Stevens-Johnson syndrome, herpes simplex or aphthous ulcer.[4]
Treatment includes identifying and stopping the causative drug and considering applying topical corticosteroid.[4]
They are common.[1] Males are affected equally to females.[3] The most likely age group is 35 to 60 years old.[3] It was first described in 1889 and the term was coined by Brocq in 1894.[3]
Signs and symptoms
It generally looks like a solitary or a few well-defined, roundish red or purplish patches which may blister.[4] It can be itchy and painful and often leaves a mark after healing.[4] The lips, genitals, and hands are often involved. The affected person feels otherwise well.[4] Common sites include hands, feet, eyelids, anogenital areas, lips, tongue and hard palate.[4] These sites may be the location of previous trauma such as an insect bite, blood test or burn.[4]
.jpg.webp) Fixed drug reaction (targeted)
Fixed drug reaction (targeted).jpg.webp) Fixed drug reaction (pigmented) on lip
Fixed drug reaction (pigmented) on lip Fixed drug reaction on hard palate
Fixed drug reaction on hard palate Fixed drug reaction (lips and penis)
Fixed drug reaction (lips and penis) Fixed drug reactio groin (erosions)
Fixed drug reactio groin (erosions).jpg.webp) Fixed drug reaction to cotrimoxazole
Fixed drug reaction to cotrimoxazole
Causes
It is a delayed type IV hypersensitivity, usually caused by antibiotics and non-steroidal anti-inflammatory drugs.[4] Medications inducing fixed drug reactions are usually those taken intermittently.[1] Medications that are commonly implicated as a cause of fixed drug reactions include the following:
Anti-microbials
- Amoxicillin[3]
- Ciprofloxacin
- Clarithromycin
- Cotrimoxazole(Trimethoprim/sulfamethoxazole)[3]
- Doxycycline[3]
- Fluconazole[4]
- Nystatin[2]
- Levofloxacin[3]
- Trimethoprim[3]
- Quinine[4]
Painkillers
Anti-hypertensive medications
Anti-epileptic drugs
Other
Vaccines
- Influenza vaccine[3]
Foods
Diagnosis
Diagnosis is by history and visualisation of the rash.[3] It may require a skin biopsy, oral challenge test with a low dose of the suspected drug or a patch test.[4]
Tests
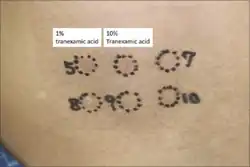 Patch test to tranexamic acid
Patch test to tranexamic acid Patch test to anti-histamines
Patch test to anti-histamines.png.webp) A. FDR, B. 30 min after oral challenge test
A. FDR, B. 30 min after oral challenge test
Histopathology
Histopathology show distinct changes in vacuoles and Civatte bodies in all levels of the epidermis.[2] The is melanin incontinence and neutrophils and eosinophils.[2]
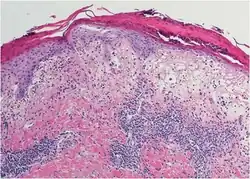 Melanin incontinence
Melanin incontinence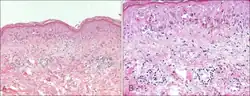 Basal vacuolation
Basal vacuolation
Treatment
Treatment includes identifying and stopping the causative drug and considering applying topical corticosteroid.[4]
Epidemiology
Fixed drug reaction is common.[1] Males are affected equally to females.[3] The most likely age group is 35 to 60 years old.[3]
History
The condition was first described in 1889 and the term was coined by Brocq in 1894.[3]
See also
References
- 1 2 3 4 5 6 7 8 James, William D.; Elston, Dirk; Treat, James R.; Rosenbach, Misha A.; Neuhaus, Isaac (2020). "6. Contact dermatitis and drug eruptions". Andrews' Diseases of the Skin: Clinical Dermatology (13th ed.). Elsevier. pp. 120–121. ISBN 978-0-323-54753-6. Archived from the original on 2021-10-16. Retrieved 2021-10-15.
- 1 2 3 4 5 6 Johnstone, Ronald B. (2017). "3. Lichenoid reaction pattern". Weedon's Skin Pathology Essentials (2nd ed.). Elsevier. p. 41. ISBN 978-0-7020-6830-0. Archived from the original on 2021-05-25. Retrieved 2021-10-16.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 Anderson, Hannah J.; Lee, Jason B. (September 2021). "A Review of Fixed Drug Eruption with a Special Focus on Generalized Bullous Fixed Drug Eruption". Medicina. 57 (9): 925. doi:10.3390/medicina57090925. Archived from the original on 2021-10-17. Retrieved 2021-10-16.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 "Fixed drug eruption | DermNet NZ". dermnetnz.org. Archived from the original on 13 August 2021. Retrieved 16 October 2021.
External links
| Classification |
|---|