Diffuse proliferative nephritis
| Diffuse proliferative nephritis | |
|---|---|
| Other names | Glomerulonephritis |
| Specialty | Nephrology |
Diffuse proliferative glomerulonephritis (DPGN) is a type of glomerulonephritis that is the most serious form of renal lesions in SLE and is also the most common, occurring in 35% to 60% of patients.[1] In absence of SLE, DPGN pathology looks more like Membranoproliferative glomerulonephritis
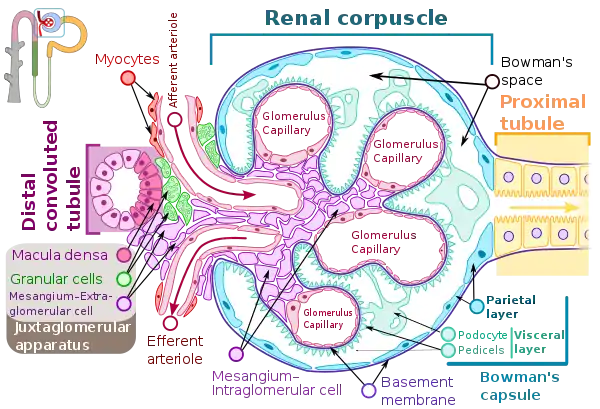
In DPGN Most of the glomeruli show endothelial and mesangial proliferation, affecting the entire glomerulus, leading to diffuse hypercellularity of the glomeruli, producing in some cases epithelial crescents that fill Bowman's space. When extensive, immune complexes create an overall thickening of the capillary wall, resembling rigid "wire loops" on routine light microscopy. Immune complexes can be visualized by staining with fluorescent antibodies directed against immunoglobulins or complement, resulting in a granular fluorescent staining pattern. Electron microscopy reveals electron-dense subendothelial immune complexes (between endothelium and basement membrane). In due course, glomerular injury in DPGN gives rise to scarring (glomerulosclerosis). Most of SLE patients with DPGN have hematuria with moderate to severe proteinuria, hypertension, and renal insufficiency.[2]
Signs and Symptoms
Symptoms can be caused directly from DPGN or from a different disease that is causing DPGN. Many of the symptoms, like edema and hypertension, occur due to the decrease in glomerular filtration rate.[3]
Patients can experience general systemic symptoms including fatigue, vomiting, nausea. These would all indicate uremia.[4]
Other patients can experience:
- Decreased urine output
- Hematuria
- Microscopic or gross
- Proteinuria
- Which will present as frothy urine
- Pedal edema
- Swelling of the feet and ankles[4]
DPGN caused by other diseases
If a patient has DPGN due to IgA nephropathy (Berger Disease) then they can experience flank pain, gross hematuria, and upper respiratory infections.
If a patient has DPGN with underlying anti-GBM then they can experience alveolar hemorrhage and respiratory issues.
If a patient has DPGN with an underlying autoimmune disease then the patient can experience photosensitivity, rash, joint pains, serositis, and oral ulcers.[4]
Cause
The cause of diffuse proliferative glomerulonephritis (DPGN) depends on the severity of the disease. DPGN is a secondary disease, in that a disease that a patient already has causes DPGN to occur. The most common associated disease of DPGN is severe systemic lupus erythematosus(SLE).[4] Specifically, Lupus nephritis class IV.[5] The other commonly associated disease is Immunoglobulin A (IgA) nephropathy. Post-infectious glomerulonephritis can also be caused by bacterial or viral infections. Streptococcal throat or skin infection is most commonly seen as the origin if glomerulonephritis is going to be caused by an infection.[6] Other causes of DPGN are endocarditis, Hepatitis B, and Hepatis C.


Mechanism/Pathophysiology
The etiology plays a role in the specific mechanism of DPGN. Usually the deposition of immune-complexes (antigen-antibody complex) that activates the complement system are involved.[4] The antibodies that form immune complexes deposits or they bind directly to the nonglomerular antibodies present. Immune-complexes are combinations of DNA, anti-dsDNA ubiquitin, and other proteins in DPGN that are associated with lupus nephritis. C1q, the first component of the complement system, encounters conformational change that leads to C3 convertase breaking C3 into C3a and C3b. C3a, C5a, IL-8 are all chemotactic factors of the activated complement system. Part of their role is to recruit polymorphonuclear cells and leukocytes. Interleukins like IL-6, tumor necrosis factor-alpha, and interferon-gamma, that cause cell injury, are released. Mesangial proliferation is caused by activated platelets.[7] Another mechanism involves antibodies formed against alpha-3 chain of collagen IV. Their deposition occurs in the sub-epithelial spaces. This causes proteinuria by damaging the basement membrane and creating a loss of negative charge. These are anionic deposits that fail to cross the membrane.[4]
Cationic deposits that cross the membrane are then deposited into sub-epithelial spaces. Then the disease advances and crescents are formed. Crescents are a combination of epithelial cells, activated macrophages, and fibrin. They lead to rupturing of small blood vessels, ultimately causing necrosis and sclerosis.[4]
Basic Summary
The glomeruli are the filters in the kidneys. When working normally they will move the waste, excess electrolytes, and unnecessary fluid from the bloodstream to the urine.[8] When a person develops DPGN, over 50% of the glomeruli (diffuse) become inflamed. There is also an increase in mesangial, epithelial, and endothelial (proliferative) cells. Inflammatory cells are also rapidly developed.[9] This causes damage to the kidneys and does not allow for proper filtration.
Diagnosis
The presentation of all types glomerulonephritis are the same.[4] If a patient is suspected to have DPGN, a blood and urine test will be done first. A urine test will be done to determine if there is protein or blood in the urine. A blood test will be to measure the levels of creatine in the blood. An ultrasound will be done to see if there is inflammation of the kidneys and to look for blockages.
A kidney biopsy is the most important diagnostic tool. With a biopsy, the sample will be looked at histologically. With this information, a proper diagnosis can be completed. There are many forms of glomerulonephritis, but under a microscope, DPGN will show increased cell count of polymorphonuclear cells, cellular crescents, and fibrinoid necrosis. A patient with DPGN will have more than 50% of their glomeruli involved.[4][5] If a patient has DPGN, that means they have an active form of glomerulonephritis.[10]
Treatment
Treatment of DPGN depends on the severity of the disease. An optimal treatment for DPGN is immunosuppressive therapy.[11] Two common immunosuppressive drugs used to treat DPGN are cyclophosphamide (CYC) and mycophenolate mofetil (MMF) if the DPGN is caused by SLE.[12] CYC and MMF both preserve the renal function in patients with SLE and DPGN.[13] CYC and MMF have been known to improve proteinuria.[13][14] There can be adverse side effects; including CYC can cause infertility in both women and men.[11] MMF has been seen to have less drug toxicity.[15] There are a variety of dosing options (oral or intravenous medications) available.[11]
If the DPGN is caused by IgA nephropathy then corticosteroids, angiotensin-converting enzyme inhibitor (ACEIs), angiotensin receptor blockers (ARBs), or both ACEIs and ARBs should be used.[15] Corticosteroids are used to suppress the immune system and to reduce inflammation.[16] ACEIs will decrease hypertension by preventing the body from creating angiotensin II, which narrows the blood vessels. ARBs block angiotensin II from acting.[17]
The patient's diet should also be changed. The patient should restrict salt intake to improve the hypertension and nephrosis. Protein restriction may reduce the progression of the disease. Fluid restriction may also be necessary if the patient is experiencing edema.
Prognosis
Prognosis is determined by the stage of the disease.[4] Aggressive therapy is recommended to avoid progressing to end-stage renal disease (ESRD), which is a strong possibility. About 10% of DPGN patients will go into ESRD.[4]
If the biopsy shows the presence of crescents, tubule-interstitial injury with inflammation atrophy and fibrosis, the outcome is worse.[4] Other factors that will influence the survival rate are the severity of proteinuria, blood urea nitrogen levels, serum creatine levels, and eGFR. Other bad prognosis features are the presence of hypertension, accelerated hematuria, and hypoalbuminemia. Males are at a higher risk factor than females. Overall, about 50% of patients with DPGN require daily dialysis within 6–12 months after disease presentation.
The percentage of glomeruli that show crescents usually correlates to the severity of the renal failure.[18][19]
The survival rate after 5 years is about 30%.[20]
Epidemiology
DPGN prevalence varies among races. Whites are the less likely to have DPGN (12-33%); while African Americans (40-69%), Hispanics (36-61%), and Asians (47-53%) are more likely to develop it.[21]
Men are more likely to develop a more aggressive disease than women. However, women are nine times more likely to develop DPGN.[22]
DPGN occurs in all age groups, but is more prevalent in women of childbearing years. Eighty-five percent of patients develop DPGN before 55 years.[22]
End Stage Renal Disease
Research Directions
In 2014 a study was completed to diagnose glomerulonephritis based on etiology. Using immunofluorescence and light microscopy, the investigators were determining the classification for the disease based on if the disease was immune complex mediated, pauci- immune, or complement mediated. They then looked at the complement factors and immunoglobulin deposits to identify the underlying cause. The aims of this study were classifying pathophysiology and to obtain a better understanding of glomerulonephritis.[24]
Much of the research within the last 10 years has been to identify the best treatment for DPGN. Other studies about DPGN from the past 10 years has included studies for other diseases that are linked to DPGN. There are no current clinical trials for DPGN happening.
Future Studies
Activating complement pathways plays a large role in mediating inflammation. The classical pathway, lectin pathway, and alternative pathway of complement are all involved in glomerulonephritis, depending on the etiology. Inactive and active complement proteins that split fragments are found in the glomeruli. There are currently drugs available that will target the complement pathway. It has been proposed that if fluorescently tagged antibodies were used to target different split products of the complement proteins, then identification of specific pathways involved and the accumulated complement proteins in the glomeruli should be achievable. This would lead to identifying which pathways and proteins drive each type of glomerulonephritis.[10]
References
- ↑ Ferri, Fred F. (2009). Ferri's Color Atlas and Text of Clinical Medicine. Elsevier Health Sciences. p. 701. ISBN 978-1416049197. Retrieved 14 November 2017.
- ↑ Robbins, Stanley L.; Kumar, Vinay (2007). Robbins basic pathology. Saunders/Elsevier. p. 142. ISBN 978-0-8089-2366-4.
- ↑ Kazi, Ahmad M.; Hashmi, Muhammad F. (2020), "Glomerulonephritis", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 32809479, retrieved 2020-12-16
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Ikhlas, Mariam; Anjum, Fatima (2020), "Diffuse Proliferative Glomerulonephritis", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 32644412, retrieved 2020-11-09
- 1 2 Weening, J. J. (2004-02-01). "The Classification of Glomerulonephritis in Systemic Lupus Erythematosus Revisited". Journal of the American Society of Nephrology. 15 (2): 241–250. doi:10.1097/01.ASN.0000108969.21691.5D. ISSN 1046-6673. PMID 14747370.
- ↑ Kambham, Neeraja (September 2012). "Postinfectious Glomerulonephritis". Advances in Anatomic Pathology. 19 (5): 338–347. doi:10.1097/PAP.0b013e31826663d9. ISSN 1072-4109. PMID 22885383. S2CID 29220743.
- ↑ Pound, S. E.; Macdonald, M. K.; Thomson, D. (1987). "Diffuse proliferative glomerulonephritis—how many types?". Histopathology. 11 (3): 227–243. doi:10.1111/j.1365-2559.1987.tb02629.x. ISSN 1365-2559. PMID 3428882. S2CID 44769947.
- ↑ "Glomerulonephritis - Symptoms and causes". Mayo Clinic. Retrieved 2020-12-16.
- ↑ "Diffuse Proliferative Glomerulonephritis: Practice Essentials, Pathophysiology, Etiology". 2020-12-05.
{{cite journal}}: Cite journal requires|journal=(help) - 1 2 Sethi, Sanjeev; Fervenza, Fernando C (2018-08-13). "Standardized classification and reporting of glomerulonephritis". Nephrology Dialysis Transplantation. 34 (2): 193–199. doi:10.1093/ndt/gfy220. ISSN 0931-0509. PMID 30124958. S2CID 52040978.
- 1 2 3 Hahn, Bevra H.; McMahon, Maureen A.; Wilkinson, Alan; Wallace, W. Dean; Daikh, David I.; FitzGerald, John D.; Karpouzas, George A.; Merrill, Joan T.; Wallace, Daniel J.; Yazdany, Jinoos; Ramsey-Goldman, Rosalind (June 2012). "American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis". Arthritis Care & Research. 64 (6): 797–808. doi:10.1002/acr.21664. PMC 3437757. PMID 22556106.
- ↑ Mok, Chi Chiu; Ying, King Yee; Ng, Woon Leung; Lee, Ka Wing; To, Chi Hung; Lau, Chak Sing; Wong, Raymond Woon Sing; Au, Tak Cheung (April 2006). "Long-term Outcome of Diffuse Proliferative Lupus Glomerulonephritis Treated with Cyclophosphamide". The American Journal of Medicine. 119 (4): 355.e25–355.e33. doi:10.1016/j.amjmed.2005.08.045. ISSN 0002-9343. PMID 16564783.
- 1 2 Mok, Chi Chiu; Ho, Carmen Tsz Kwan; Siu, Yui Pong; Chan, Kwok Wah; Kwan, Tsz Hoi; Lau, Chak Sing; Wong, Raymond W.S.; Au, Tak Cheung (August 2001). "Treatment of diffuse proliferative lupus glomerulonephritis: A comparison of two cyclophosphamide-containing regimens". American Journal of Kidney Diseases. 38 (2): 256–264. doi:10.1053/ajkd.2001.26084. PMID 11479150.
- ↑ Ding, Lei; Zhao, Minghui; Zou, Wanzhong; Liu, Yuchun; Wang, Haiyan (February 2004). "Mycophenolate mofetil combined with prednisone for diffuse proliferative lupus nephritis: a histopathological study". Lupus. 13 (2): 113–118. doi:10.1191/0961203304lu513oa. ISSN 0961-2033. PMID 14995004. S2CID 25408973.
- 1 2 Chan, Tak-Mao; Tse, Kai-Chung; Tang, Colin Siu-On; Mok, Mo-Yin; Li, Fu-Keung (2005-04-01). "Long-Term Study of Mycophenolate Mofetil as Continuous Induction and Maintenance Treatment for Diffuse Proliferative Lupus Nephritis". Journal of the American Society of Nephrology. 16 (4): 1076–1084. doi:10.1681/ASN.2004080686. ISSN 1046-6673. PMID 15728784.
- ↑ Rice, J. Bradford; White, Alan G.; Scarpati, Lauren M.; Wan, George; Nelson, Winnie W. (November 2017). "Long-term Systemic Corticosteroid Exposure: A Systematic Literature Review". Clinical Therapeutics. 39 (11): 2216–2229. doi:10.1016/j.clinthera.2017.09.011. PMID 29055500.
- ↑ Li, Edmond CK; Heran, Balraj S; Wright, James M (2014-08-22). Cochrane Hypertension Group (ed.). "Angiotensin converting enzyme (ACE) inhibitors versus angiotensin receptor blockers for primary hypertension". Cochrane Database of Systematic Reviews (8): CD009096. doi:10.1002/14651858.CD009096.pub2. PMC 6486121. PMID 25148386.
- ↑ Gupta, Vibhanshu; Sachdeva, Sandeep; Khan, Anwar Salamat; Haque, Shahzad Faisul (March 2012). "Diffuse proliferative crescentic lupus nephritis with normal renal function". Saudi Journal of Kidney Diseases and Transplantation. 23 (2): 343–345. ISSN 1319-2442. PMID 22382232.
- ↑ Whitworth, Judith A.; Morel-Maroger, L.; Mignon, F.; Richet, G. (1976). "The Significance of Extracapillary Proliferation". Nephron. 16 (1): 1–19. doi:10.1159/000180578. ISSN 1423-0186. PMID 1244562.
- ↑ Polenaković, M.; Grcevska, L. (1992). "Survival rate of patients with glomerulonephritis". Acta Medica Croatica: Casopis Hravatske Akademije Medicinskih Znanosti. 46 (1): 15–20. ISSN 1330-0164. PMID 1380354.
- ↑ Korbet, Stephen M.; Schwartz, Melvin M.; Evans, Joni; Lewis, Edmund J. (2007-01-01). "Severe Lupus Nephritis: Racial Differences in Presentation and Outcome". Journal of the American Society of Nephrology. 18 (1): 244–254. doi:10.1681/ASN.2006090992. ISSN 1046-6673. PMID 17167111.
- 1 2 Vachvanichsanong, P.; Dissaneewate, P.; McNeil, E. (2009-04-25). "Diffuse proliferative glomerulonephritis does not determine the worst outcome in childhood-onset lupus nephritis: a 23-year experience in a single centre". Nephrology Dialysis Transplantation. 24 (9): 2729–2734. doi:10.1093/ndt/gfp173. ISSN 0931-0509. PMID 19395731.
- ↑ "Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2017;7:1–59". Kidney International Supplements. 7 (3): e1. December 2017. doi:10.1016/j.kisu.2017.10.001. ISSN 2157-1716. S2CID 58992243.
- ↑ Sethi, Sanjeev (April 2014). "Etiology-Based Diagnostic Approach to Proliferative Glomerulonephritis". American Journal of Kidney Diseases. 63 (4): 561–566. doi:10.1053/j.ajkd.2013.11.019. ISSN 0272-6386. PMID 24387793.