Tubo-ovarian abscess
| Tubo-ovarian abscesses(TOA) | |
|---|---|
| Other names: Salpingitis[1] | |
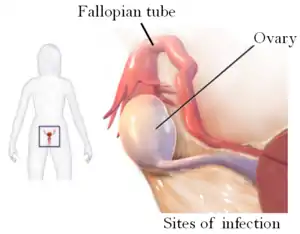 | |
| Drawing showing the sites of Tubo-ovarian abscess | |
| Specialty | Gynaecology |
| Symptoms | Lump in the pelvis, low down tummy ache, fever, vaginal discharge[1] |
| Complications | Peritonitis[2] |
| Usual onset | Young women[1] |
| Causes | Anaerobic bacteria[1] |
| Risk factors | IUD insertion, previous PID, multiple sexual partners,[2] diabetes[1] |
| Diagnostic method |
|
| Differential diagnosis | Appendicitis, diverticulitis, pelvic inflammatory disease, ovarian torsion, inflammatory bowel disease, ectopic pregnancy, ruptured ovarian cyst, bladder infection, kidney infection[2] |
Tubo-ovarian abscess (TOA), is a mass of inflammation in the ovary and fallopian tube, occurring typically after an upper genital tract infection in females of childbearing age.[1] It presents as a pelvic lump, low down tummy ache, vaginal discharge and fever.[1] There may be nausea and abnormal vaginal bleeding.[1] It is a late complication of pelvic inflammatory disease (PID), and can be life-threatening if it ruptures and results in sepsis.[2]
It consists of a walled off mass of pus with defined boundaries that forms in the fallopian tube and ovary.[2] It tends to occur following upper genital tract infection and [[PID}} in females of reproductive age who have sex.[2] It may involve adjacent pelvic organs.[1] A TOA can also develop as a complication of a hysterectomy.[3]: 103 Though rare, TOA can occur without a preceding episode of PID or sexual activity.[4][5] Infection from the cervix or vaginal spread up through the inner lining of the uterus and the fallopian tubes into the peritoneal cavity where it forms a walled-off mass, and often results in peritonitis.[2] A nearby infection such as of the appendix may less commonly extend to form a tubo-ovarian abscess.[2] Other risk factors include IUD insertion, multiple sexual partners, previous PID, and pelvic organ cancer.[2] It may be associated with diabetes and endometriosis.[1] Conditions that may appear similar include appendicitis, diverticulitis, pelvic inflammatory disease, ovarian torsion, inflammatory bowel disease, ectopic pregnancy, ruptured ovarian cyst, bladder infection, and kidney infection.[2] The most frequently reported bacteria isolated from tubo-ovarian abscessess include Escherichia coli, Bacteroides fragilis, Peptostreptococcus, Peptococcus, and aerobic streptococci.[2]
There maybe yellow-green discharge seen from the cervix when looking with a speculum.[2] It may hurt during an internal examination or when the cervix is moved.[2] A blood test usually reveals an elevated white blood cell count.[2] Other tests include pregnancy test, culture of urine, cervical discharge and blood, as well as a wet mount of vaginal discharge for clue cells.[2] An assessment of the abscess can be made using medical imaging; ultrasound, CT scan, MRI.[2] Diagnosis and assessment may be completed with a laparoscopy, during which it can be drained.[2] Treatment is initially with antibiotics given by injection.[2]
The cost of treatment in the United States is approximately $2,000 per patient, which equals about $1.5 billion annually.[6]
Signs and symptoms

The signs and symptoms of tubo-ovarian abscess (TOA) are the same as with pelvic inflammatory disease (PID) with the exception that the abscess can be found with magnetic resonance imaging (MRI), sonography and x-ray.[6][7] It also differs from PID in that it can create symptoms of acute-onset pelvic pain.[8] Typically this disease is found in sexually active women.[4][9] Tubo-ovarian abscess can mimic abdominal tumours.[10]
Complications
Complications of TOA are related to the possible removal of one or both ovaries and fallopian tubes. Without these reproductive structures, fertility can be affected. Surgical complications can develop and include:
- Allergic shock due to anesthetics
- A paradoxical reaction to a drug
- Infection
Cause
The development of TOA is thought to begin with the pathogens spreading from the cervix to the endometrium, through the salpinx, into the peritoneal cavity and forming the tubo-ovarian abscess with (in some cases) pelvic peritonitis. TOA can develop from the lymphatic system with infection of the parametrium from an intrauterine device (IUD).[6] Bacteria recovered from TOAs are Escherichia coli, Bacteroides fragilis, other Bacteroides species, Peptostreptococcus, Peptococcus, and aerobic streptococci.[11] Long term IUD use is associated with TOA.[12] Actinomyces is also recovered from TOA.[12]
| Genus | species | Gram stain | form | genome sequenced | reference |
|---|---|---|---|---|---|
| Neisseria gonorrhoeae | spp. | + | cocci | [6][13] | |
| Chlamydia trachomatis | spp. | + | intracellular | [6][13] | |
| Mycoplasma genitalium | spp. | + | bacillus | [13] | |
| Mycoplasma hominis | [13] | ||||
| Ureaplasma urealyticum | + | bacillus | [13] | ||
| Escherichia coli | + | bacillus | X | [4][11][13] | |
| Corynebacterium jeikeium | + | bacillus | X | [13] | |
| Bacteroides fragilis | + | bacillus | X | [11][13] | |
| Lactobacillus | jensenii | + | bacillus | [13] | |
| Cutibacterium acnes | + | bacillus | [13] | ||
| Haemophilus influenzae | + | bacillus | [13] | ||
| Streptococcus pneumoniae | + | cocci | [13] | ||
| Streptococcus constellatus | + | cocci | [11][13] | ||
| Prevotella bivia | + | bacillus | [13] | ||
| Fusobacterium nucleatum | + | bacillus | [13] | ||
| Enterococcus faecium | + | cocci | [13] | ||
| Actinomyces neuii | + | bacillus | X | [13] | |
| Lactobacillus | delbrueckii | + | bacillus | [13] | |
| Streptococcus intermedius | + | cocci | [11][13] | ||
| Eikenella corrodens | + | bacillus | X | [13] | |
| Abiotrophia | + | bacillus | X | [4] | |
| Granulicatella | + | bacillus | X | [4] | |
Diagnosis
Laparoscopy and other imaging tools can visualize the abscess. Physicians are able to make the diagnosis if the abscess ruptures when the woman begins to have lower abdominal pain that then begins to spread. The symptoms then become the same as the symptoms for peritonitis. Sepsis occurs, if left untreated.[3]: 103 Ultrasonography is a sensitive enough imaging tool that it can accurately differentiate between pregnancy, hemorrhagic ovarian cysts, endometriosis, ovarian torsion, and tubo-ovarian abscess. Its availability, the relative advancement in the training of its use, its low cost, and because it does not expose the woman (or fetus) to ionizing radiation, ultrasonography an ideal imaging procedure for women of reproductive age.[8]
Prevention
Risk factors have been identified which indicate what women will be more likely to develop TOA. These are: increased age, IUD insertion, chlamydia infection, and increased levels of certain proteins (CRP and CA-125) and will alert clinicians to follow up on unresolved symptoms of PID.[14]
Treatment
Treatment for TOA differs from PID in that some clinicians recommend patients with tubo-ovarian abscesses have at least 24 hours of inpatient parenteral treatment with antibiotics, and that they may require surgery.[6][15] If surgery becomes necessary, pre-operative administration of broad-spectrum antibiotics is started and removal of the abscess, the affected ovary and fallopian tube is done. After discharge from the hospital, oral antibiotics are continued for the length of time prescribed by the physician.[3]: 103
Treatment is different if the TOA is discovered before it ruptures and can be treated with IV antibiotics. During this treatment, IV antibiotics are usually replaced with oral antibiotics on an outpatient basis. Patients are usually seen three days after hospital discharge and then again one to two weeks later to confirm that the infection has cleared.[3]: 103 Ampicillin/sulbactam plus doxycycline is effective against C. trachomatis, N. gonorrhoeae, and anaerobes in women with tubo-ovarian abscess. Parenteral Regimens described by the Centers for Disease Control and prevention are Ampicillin/Sulbactam 3 g IV every 6 hours and Doxycycline 200 mg orally or IV every 24 hours, though other regiments that are used for pelvic inflammatory disease have been effective.[16]
Epidemiology
The epidemiology of TOA is closely related to that of pelvic inflammatory disease which is estimated to one million people yearly.[17]
References
- 1 2 3 4 5 6 7 8 9 10 11 WHO Classification of Tumours Editorial Board, ed. (2020). "4. Tumours of the fallopian tube". Female genital tumours: WHO Classification of Tumours. Vol. 4 (5th ed.). Lyon (France): International Agency for Research on Cancer. p. 225. ISBN 978-92-832-4504-9. Archived from the original on 2022-06-17. Retrieved 2022-07-29.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 Kairys, Norah; Roepke, Clare (2022). "Tubo-Ovarian Abscess". StatPearls. StatPearls Publishing. PMID 28846347. Archived from the original on 2022-07-28. Retrieved 2022-07-26.
- 1 2 3 4 Hoffman, Barbara (2012). Williams gynecology. New York: McGraw-Hill Medical. ISBN 9780071716727.
- 1 2 3 4 5 Goodwin, K.; Fleming, N.; Dumont, T. (2013). "Tubo-ovarian Abscess in Virginal Adolescent Females: A Case Report and Review of the Literature". Journal of Pediatric and Adolescent Gynecology. 26 (4): e99–e102. doi:10.1016/j.jpag.2013.02.004. ISSN 1083-3188. PMID 23566794.
- ↑ Ho, Jeh Wen; Angstetra, D.; Loong, R.; Fleming, T. (2014). "Tuboovarian Abscess as Primary Presentation for Imperforate Hymen". Case Reports in Obstetrics and Gynecology. 2014: 1–3. doi:10.1155/2014/142039. ISSN 2090-6684. PMC 4009186. PMID 24822139.
- 1 2 3 4 5 6 Pelvic inflammatory disease. American Family Physician, Vol. 85, No. 8. (15 April 2012), pp. 791-796 by Margaret Gradison
- ↑ "CDC - Pelvic Inflammatory Disease - 2010 STD Treatment Guidelines". Archived from the original on 2015-02-22. Retrieved 2015-05-16.
- 1 2 Dupuis, Carolyn S.; Kim, Young H. (2015). "Ultrasonography of adnexal causes of acute pelvic pain in pre-menopausal non-pregnant women". Ultrasonography. 34 (4): 258–267. doi:10.14366/usg.15013. ISSN 2288-5919. PMC 4603210. PMID 26062637.
- ↑ Cho, Hyun-Woong; Koo, Yu-Jin; Min, Kyung-Jin; Hong, Jin-Hwa; Lee, Jae-Kwan (2015). "Pelvic Inflammatory Disease in Virgin Women with Tubo-ovarian Abscess: A Single-center Experience and Literature Review". Journal of Pediatric and Adolescent Gynecology. 30 (2): 203–208. doi:10.1016/j.jpag.2015.08.001. ISSN 1083-3188. PMID 26260586.
- ↑ Lim, Andy; Pourya, Pouryahya; Lim, Alvin (2020). "Tubo-ovarian Abscess Masquerading as Dual Tumours". OSP Journal of Case Reports. 2 (2). doi:10.26180/5ed852773f47e. Archived from the original on 4 June 2020. Retrieved 4 June 2020.
- 1 2 3 4 5 Landers, D. V.; Sweet, R. L. (1983). "Tubo-ovarian Abscess: Contemporary Approach to Management". Clinical Infectious Diseases. 5 (5): 876–884. doi:10.1093/clinids/5.5.876. ISSN 1058-4838. PMID 6635426.
- 1 2 Lentz, Gretchen (2013). Comprehensive gynecology. Philadelphia: Mosby Elsevier. p. 558. ISBN 9780323069861.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Dessein, Rodrigue; Giraudet, Géraldine; Marceau, Laure; Kipnis, Eric; Galichet, Sébastien; Lucot, Jean-Philippe; Faure, Karine; Munson, E. (2015). "Identification of Sexually Transmitted Bacteria in Tubo-Ovarian Abscesses through Nucleic Acid Amplification: TABLE 1". Journal of Clinical Microbiology. 53 (1): 357–359. doi:10.1128/JCM.02575-14. ISSN 0095-1137. PMC 4290956. PMID 25355760.
- ↑ Lee, Suk Woo; Rhim, Chae Chun; Kim, Jang Heub; Lee, Sung Jong; Yoo, Sie Hyeon; Kim, Shin Young; Hwang, Young Bin; Shin, So Young; Yoon, Joo Hee (2015). "Predictive Markers of Tubo-Ovarian Abscess in Pelvic Inflammatory Disease". Gynecologic and Obstetric Investigation. 81 (2): 97–104. doi:10.1159/000381772. ISSN 0378-7346. PMID 25926103. S2CID 27186672.
- ↑ Lentz, Gretchen (2013). Comprehensive gynecology. Philadelphia: Mosby Elsevier. p. 584. ISBN 9780323069861.
- ↑ "CDC - Pelvic Inflammatory Disease - 2010 STD Treatment Guidelines". www.cdc.gov. Archived from the original on 2011-02-09.
- ↑ "PID Epidemiology". Center for Disease Control. Archived from the original on 2015-02-22. Retrieved 2015-05-21.
External links
| Classification | |
|---|---|
| External resources |